

Translate this page into:
Correlation of upper lip morphology to smile: A photographic study
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aims and Objective
The purpose of this study was to examine different components of a smile in subjects with class I occlusion and to formulate a comprehensive photographic analysis of a smile. This study was designed to find a correlation between upper lip elevation and retraction with upper lip morphology during smiling among male and female groups.
Materials and Methods
Lateral cephalogram and standardized frontal photographs were taken at rest and smiling.
Results
A significant sexual dimorphism was apparent in several of the parameters studied. Middle portion of lower border of upper lip (MUL’-MUL) rose significantly higher by 0.91 mm in the male group than in the female group, during smiling (P = 0.003). Decrease in vermillion display (VE-VE’) was significantly higher in the male group than the in female group by 0.668 mm (P = 0.021).
Conclusion
This comprehensive study of lip mobility, when applied to a larger population can enable us to further evaluate the correlation between lip morphology and mobility.
Keywords
Lateral cephalogram
lip morphology
vermillion display

INTRODUCTION
An attractive smile in modern society is considered as a valuable asset.[1,2] A smile is considered a universal friendly greeting in all cultures.[3] Recent publications have focused attention on evaluation of the smile as a primary esthetic factor in orthodontic diagnosis.[4-6] There has been a paradigm shift from evaluating only static soft-tissue relationships to a dynamic one while formulating orthodontic treatment goals.
The upper and lower lips frame the display zone of the smile.[2] Though Calvin Case advocated facial esthetic evaluation as an important factor in orthodontic diagnosis in the early 20th century,[7] the nonextraction stance of Edward Angle and the advent of cephalometrics led the specialty through an era of focusing on hard tissue goals for orthodontic treatment.[8] The re-emergence of soft-tissue esthetics evaluation as a factor in orthodontic treatment planning emphasized relaxed lip posture as an essential element of proper diagnosis. Burstone[9] advocated examining first the relaxed lip and then the closed lip posture primarily for determining proper positioning of the incisors. More dynamic measures, taken during activities like smiling,[10-12] were considered difficult to reproduce and, therefore, unreliable.
Cephalometric radiograph, a helpful diagnostic tool does not record lip tooth relationships during speech and smiling. Clinical observation and photographs of the face at rest and smile are necessary to obtain this valuable information.[13,14] Through the smile photograph, the clinician can identify and analyze anterior tooth and adjacent soft-tissue relationship.
The purpose of this study was to examine different components of a smile in subjects with class I occlusion and to formulate a comprehensive photographic analysis of a smile. This would help clinicians in analyzing the type of treatment mechanics they could use to correct most of the malocclusions.
MATERIALS AND METHODS
This study was designed to find a correlation between upper lip morphology to lip elevation at rest and on smiling among male and female groups using lateral cephalogram and standardized frontal photographs taken at rest and smiling. The study was conducted in the Department of Orthodontics and Dentofacial Orthopedics, Bharati Vidyapeeth Deemed University’s Dental College and Hospital, Pune, Maharashtra, India.
The components of inclusion criteria were adult subjects aged 18-25 years with straight profile and class I molar relationship, overbite ranging from 1 to 3 mm and with over jet from 1 to 3 mm. The exclusion criteria were history of orthodontic treatment, orthognathic surgery, and missing or replaced teeth. A total of 53 subjects fulfilling the above criteria was selected. All subjects were explained the nature and design of the study. Consents were obtained from them on a prescribed format.
A lateral cephalogram was made for each subject on KODAK TROPHY, 500C OPG and KODAK 8000C cephalometric machine in the Department of Oral Medicine and Dental Radiology, Bharati Vidyapeeth Deemed University’s Dental College and Hospital, Pune, Maharashtra, India. Exposure time for each cephalogram was 2.25 s and the magnification was 1:1.22. Standardized photographs from the frontal view at rest and on smiling were taken using a digital camera mounted on a tripod at eye level of the subject with a fixed distance of 3 feet [Figure 1].
- Frontal photograph at rest
Frontal photograph was taken when the lips were at rest position. To obtain the rest position, subjects were made to sit straight in front of the camera and close to the wall keeping ala tragus line parallel to the floor. Subjects were asked to say “Mississippi” and then keep the lips in that position [Figure 2]. To achieve the maximum smiling position, subjects were asked to smile maximum and reproduce the same smile at least twice successively [Figure 3]. Photographs were taken in this position. In this way, most subjects easily attained a reproducible maximum smile.
- Photographic setup

- Frontal photograph on smiling
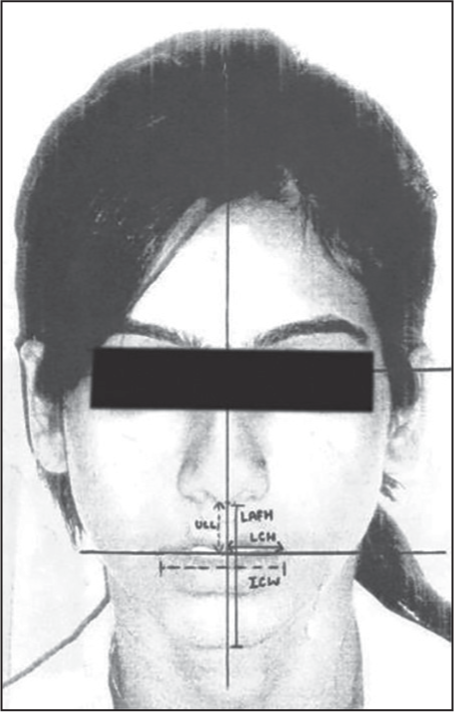
With a 0.5 mm Hb lead pencil, following lines were made on a matte acetate paper (0.003 inches thick, Garware) which was attached to the photographs. Outline of face, lips, and eyes were traced on the photographs. Outline of upper lip, nose, maxillary bone, and FH plane was traced on the lateral cephalogram.
Linear millimetric measurements traced on photographs are
Upper lip length (ULL): Distance measured from subnasale to the inferior border of the upper lip.
Lower anterior face height (LAFH): Distance measured from subnasale to soft-tissue menton.
Vermillion display: Distance between labial superior and stomion superior. (VE) at rest, (VE’) on smiling.
Right commissure position: Horizontal distance of right commissure from midline (“M” line). (RCH) at rest, (RCH’) on smiling.
Left commissure position: Horizontal distance of left commissure from midline (“M” line). (LCH) at rest, (LCH’) on smiling.
Left commissure position: Vertical distance of the left commissure from “H” line. (LCV) at rest, (LCV’) on smiling.
Middle portion of upper lip from “M” line: (MUL) at rest, (MUL’) on smiling.
Intercommissure distance: Distance between the right and the left commissures. Intercommissure width (ICW) at rest, (ICW’) on smiling.
Linear millimetric measurements on radiographs
Upper lip thickness (ULLM): Horizontal distance is measured at maximum lip contour parallel to the FH plane.
The data were tabulated in the master charts and was subjected to statistical analysis using SPSS 13.0 software (IBM Inc.)The mean difference, standard deviation, and the coefficient of correlations (CC) were calculated for all the variables.
RESULTS
A significant sexual dimorphism was apparent in several of the parameters studied [Table 1]. Middle portion of lower border of upper lip (MUL’-MUL) rose significantly higher by 0.91 mm in the male group than in the female group, during smiling (P = 0.003). Decrease in vermillion display (VE-VE’) was significantly higher in the male group than the in female group by 0.668 mm (P = 0.021).
| Linear changes in lip movement | Sex | Mean | SD | P |
|---|---|---|---|---|
| RCH’-RCH | Male | 4.21 | 1.45 | 0.602 |
| Female | 4.43 | 1.51 | ||
| LCH’-LCH | Male | 3.67 | 1.33 | 0.235 |
| Female | 4.17 | 1.63 | ||
| ICW’-ICW1 | Male | 7.81 | 2.42 | 0.405 |
| Female | 8.39 | 2.61 | ||
| RCV’-RCV1 | Male | 5.40 | 1.49 | 0.068 |
| Female | 4.74 | 1.05 | ||
| LCV’-LCV1 | Male | 5.44 | 1.52 | 0.075 |
| Female | 4.74 | 1.28 | ||
| MUL’-MUL1 | Male | 3.96 | 1.17 | 0.003* |
| Female | 3.06 | 0.90 | ||
| VE-VE’ | Male | 1.02 | 1.07 | 0.021* |
| Female | 0.36 | 0.97 |
*Signifi cant (P < 0.05). SD – Standard deviation; ICW – Intercommissure width
The result showed that the mean ICW was greater in the male group than in the female group by 2.45 mm. It was directly proportional to the ULL in both sexes, that is, male (CC = 0.542) and female (CC = 0.404). This relation was statistically significant (P ≤ 0.001). It was observed that the ICW has a positive correlation to the LAFH in the males (CC = 0.694) and females (CC = 0.552), relation being statistically significant.
Table 2 shows the mean and standard deviations of the various parameters at rest positions in male and female groups. All the parameters were found to be significantly different between males and females. LAFH was significantly higher in the male group than in the female group by 4.7 mm (P ≤ 0.001). The ULL was significantly more in the male group than in the female group by 2.1 mm (P ≤ 0.001). At maximum lip contour upper lip thickness was significantly more in the male group than in the female group by 2.1 mm (P = 0.007).
| Rest position | Group | n | Mean | SD | P |
|---|---|---|---|---|---|
| ULL | Male | 27 | 12.13 | 1.38 | <0.001 |
| Female | 26 | 10.05 | 1.21 | ||
| Intercommissure distance | Male | 27 | 27.38 | 2.34 | <0.001 |
| Female | 26 | 24.85 | 1.98 | ||
| LAFH | Male | 27 | 37.27 | 3.66 | <0.001 |
| Female | 26 | 32.57 | 3.60 | ||
| ULLM | Male | 27 | 14.17 | 3.55 | 0.007 |
| Female | 26 | 12.04 | 1.69 |
ULL – Upper lip length; LAFH – Lower anterior face height; ULLM – Upper lip thickness at maximum lip contour; SD – Standard deviation
Change of vermillion display shows no significant correlation with ULL in male and female groups separately. The right commissure retraction and left commissure retraction shows no correlation to lip thickness in the male, female as well as combined groups. The mean intercommissure width was greater in males than in females.
Table 3 shows the correlation of lip thickness with lip retraction in a vertical direction on smiling. It also shows lip elevation at commissures and the midpoint is not related to lip thickness in the male, female and combined group. Table 4 shows the correlation between upper lip thickness and change in vermillion display. Change of vermillion display shows no correlation to the upper lip thickness in the male, female, and combined group.
| Lip retraction in vertical direction | Group | n | Upper lip thickness | |
|---|---|---|---|---|
| Correlation coeffi cient | P | |||
| RCV’-RCV | Male | 26 | 0.045 | 0.828 |
| Female | 27 | −0.021 | 0.916 | |
| Combined | 53 | 0.117 | 0.403 | |
| LCV’-LCV | Male | 26 | −0.070 | 0.733 |
| Female | 27 | 0.058 | 0.774 | |
| Combined | 53 | 0.062 | 0.659 | |
| MUL’-MUL | Male | 26 | 0.014 | 0.947 |
| Female | 27 | −0.115 | 0.567 | |
| Combined | 53 | 0.130 | 0.353 | |
| Change in vermillion display | Group | n | Upper lip thickness | |
|---|---|---|---|---|
| Correlation coeffi cient | P | |||
| VE’-VE | Male | 26 | 0.088 | 0.667 |
| Female | 27 | −0.102 | 0.611 | |
| Combined | 53 | 0.141 | 0.314 | |
DISCUSSION
Lip analysis is helpful in evaluating dentofacial composition and establishing smile design. Lips create boundaries of smile. Understanding the lip morphology and mobility can be helpful in meeting patient’s expectations and determining the criteria of successful treatment results.
There are three aspects of lip morphology that should be considered, that is, lip width, fullness, and symmetry.[15-17] In the present study, lip morphology and mobility have been analyzed. Lateral cephalogram has been included to measure lip thickness, and frontal photographs have been used to evaluate lip mobility.
When ULL was correlated to the ICW, a positive moderate correlation was found in males (CC = 0.542) and females (CC = 0.404). Similarly, ICW was also correlated with lower facial height (LAFH - subnasale to soft-tissue menton). The finding reveals that the intercommissure distance is moderately correlated and is highly significant in males (P ≤ 0.001) and females (P = 0.003). It means that as the facial proportions increase, the intercommissure width and LAFH increase proportionally.
The upward movement of upper lip at the midline was compared between male and female group using unpaired t-test as shown in Table 2. The findings showed that the elevation of the middle portion was more in male group than in female group. The average upward movement in male was 3.96 mm and female was 3.055 (P = 0.003). These findings are in contrast to Peck et al.[18] who found that the upper lip smile line was 1.5 mm more superior in the female sample than in the male sample (P < 0.01). A study done by McAlister et al.,[19] findings also showed that women have higher smile-line than men.
In the present study, an attempt was also made to correlate lip elevation at both commissures and lip thickness. No statistically significant correlation was found in either sex. McAlister et al. also found no correlation of lip elevation to lip thickness. The only difference in the studies was that the upper lip thickness of the levator labii superioris or zygomaticus major muscles were measured by the ultrasound scan whereas in the present study lip thickness was measured on lateral cephalograms.
Change of vermillion exposure showed no significant correlation to the upper lip thickness as shown in Table 4. The mean of change in vermillion exposure at rest and during smiling was compared between male and female group. The change was found to be greater in male group (1.019 mm) than in female (0.035 mm) group (P = 0.021). This could be due to a greater elevation of the lip in the middle portion of upper lip in males than in females. The greater elevation could cause greater stretch in the middle portion thereby causing greater change in vermillion display in males than in females.
Change in ICW while smiling (ICW’-ICW) was compared in both groups. It was found that smile is broader in female group than in male group, however, it is not statistically significant (P = 0.405). The mean of LAFH was more in male group (37.2 mm) than in female group (32.5 mm) as also was the mean intercommissure distance (ICW). This could be attributed to larger body proportions in general and face in particular in males than in females. ULL was found to be significantly larger in males than in females (P ≥ 0.001). Findings from this study are in accordance with the study by Fernández-Riveiro et al.[20] Peck et al. found similar results, attributing it to larger body proportions in males than in females.[18]
Lip thickness was also found to be more in males than in females. This could be due to the muscle mass. However, in a study done by McAlister et al.,[19] women have significantly thicker zygomaticus major muscles.
This study has been an attempt to understand how the smile line is related to lip morphology in normal subjects and also the variation in different smile parameters between male and female subjects, thereby helping us in proper diagnosis and treatment planning.
CONCLUSIONS
This study of lip mobility and morphology provides a useful diagnostic tool in smile design during orthodontic treatment. This comprehensive study of lip mobility, when applied to a larger population, can enable us to further evaluate the correlation between lip morphology and mobility.
References
- Dynamic smile analysis in young adults. Am J Orthod Dentofacial Orthop. 2007;132:307-15.
- [Google Scholar]
- Perceptions of dental professionals and laypersons to altered dental aesthetics: Asymmetric and symmetric situations. Am J Orthod Dentofacial Orthop. 2006;130:141-51.
- [Google Scholar]
- Photographic and videographic assessment of smile:objective and subjective evaluations of posed and spontaneous smiles. Am J Orthod Dentofacial Orthop. 2013;144:793-801.
- [Google Scholar]
- The myth of Janus: Orthodontic progress faces orthodontic history. Am J Orthod Dentofacial Orthop. 2003;123:594-6.
- [Google Scholar]
- Lip posture and its significance in treatment planning. Am J Orthod. 1967;53:262-84.
- [Google Scholar]
- Hard- and soft-tissue contributions to the esthetics of the posed smile in growing patients seeking orthodontic treatment. Am J Orthod Dentofacial Orthop. 2008;133:491-8.
- [Google Scholar]
- Photographic and videographic assessment of the smile: objective and subjective evaluations of posed and spontaneous smiles. Am J Orthod Dentofacial Orthop. 2013;144:793-801.
- [Google Scholar]
- Esthetics and Smile Characteristics at Rest and during Smile. J Ind Orthod Soc. 2012;46:17-25.
- [Google Scholar]
- The importance of Incisor Positioning in Esthetic Smile: The Smile Arc. Am J Orthod. 2001;120:98-111.
- [Google Scholar]
- Interview on facial esthetics with Dr. Anthony A. Gianelly. Prog Orthod. 2006;7:66-75.
- [Google Scholar]
- Some vertical lineaments of lip position. Am J Orthod Dentofacial Orthop. 1992;101:519-24.
- [Google Scholar]
- An ultrasound investigation of the lip levator musculature. Eur J Orthod. 1998;20:713-20.
- [Google Scholar]
- Linear photogrammetric analysis of the soft tissue facial profile. Am J Orthod Dentofacial Orthop. 2002;122:59-66.
- [Google Scholar]




