
Translate this page into:
Archwise distraction appliance: A novel approach for developing facial and dental esthetics in cleft lip and palate patients
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cleft lip and palate (CLP) is defined as a congenital deformity caused by failed fusion of medial and lateral palatine processes during 4-12th weeks of embryogenesis, resulting in an open communication between oral and nasal cavities. In CLP patients, maxillary hypoplasia, velopharyngeal insufficiency, and alveolar clefts are the major issues that have to be taken care of after labiopalatal reconstruction. Rather than several consecutive operations, such as bone-grafting and orthognathic surgery, alveolar distraction can be a better treatment option in many cases. Archwise Distraction Appliance (AWDA) is a rigid, tooth-borne, custom-made appliance that is developed to control the distraction vector with double archwire system. Our experiences show that the AWDA is a successful appliance in cases of distraction osteogenesis. Moreover, alveolar distraction has significant advantages over conventional treatment modalities for CLP patients.
Keywords
Alveolar distraction
intraoral arch-wise distraction
arch-wise distraction appliance

[SHOW_RELATED_PUBMED_ARTICLES]
INTRODUCTION
Cleft lip and palate (CLP) is defined as a congenital deformity caused by failed fusion of medial and lateral palatine processes during 4-12th weeks of embryogenesis. This results with an open communication between oral and nasal cavities. Although the exact etiology is unknown, it is thought to be a multifactorial defect including both genetic and environmental factors.
Treatment of CLP patients starts from birth onward and continues until late adolescence. This requires the care of a crowded team that includes orthodontist, speech therapist, plastic surgeon, neurologist, ENT specialist, pedodontist, prosthodontist, pediatrician, and a pedagogue. The role of the orthodontists usually begins after birth, either with passive feeding plates or active preoperative orthopedics in babies with complete clefts.
Maxillary hypoplasia, velopharyngeal insufficiency (VPI), and alveolar clefts are the major issues that have to be taken care of after labiopalatal reconstruction. Rather than several consecutive operations, such as bone-grafting and orthognathic surgery, alveolar distraction can be a better treatment option in many cases. We will not mention the general consequences of orthognathic surgeries here. However, one specific limitation of maxillary advancement in CLP patients is that velopharyngeal distance increases postsurgically. Especially in patients with already existing VPI or in borderline cases, orthognathic surgery may not be the best option. In such cases, intraoral alveolar distraction can be more beneficial for the patient.
Distraction osteogenesis (DO) was first performed by Codivilla,[1] and became widely known after Ilizarov described details of the method and developed innovative devices for this purpose.[2-4] The procedure can be summarized as a periodical distraction of two bone segments that are separated with a smooth osteotomy cut. It depends on the principle of tissue regeneration parallel to the distraction vector between two bone segments. Stretching of the tissues that bone segments are connected to stimulate not only bone regeneration between these two segments, but also regeneration and adaptation of neurovascular bundle, muscles, and surrounding soft tissue.[5] The process begins with the osteotomy of the segments and callus formation in between them, followed by gradual traction forces applied to the bone segments. This creates tensional stress in the callus and continues as long as the tissue is stretched. The stretching activity induces new bone formation and the adaptive soft tissue changes such as formation of mucosa, muscle, nerve, vascular structures, connective tissue, and lymphatic vessels.
Alveolar distraction (first introduced by Ilizarov[2,3]) is a form of bone transport and includes the transport of healthy bone segment to the neighboring defect site. Depending on the vector of force and the movement, it can be defined as vertical or horizontal. In CLP cases, healthy alveolar bone segment(s) (including the teeth) are distracted toward the defect site, until two alveolar segments come in contact. Moreover, sagittal advancement to correct maxillary hypoplasia is also possible.
ARCHWISE DISTRACTION APPLIANCE
In 2000, Liou et al. applied horizontal alveolar DO to CLP patients for the first time.[6] He used a custom-made distraction appliance to restore the alveolar defects. However, in many studies, transporting the alveolar bone in the curvilinear fashion has been a challenge. Contemporarily, a new appliance can overcome this challenge: Archwise Distraction Appliance (AWDA).
Archwise Distraction Appliance is a rigid, tooth-borne, custom-made appliance that is developed to control the distraction vector with double archwire system. The appliance consists of three major parts: Cr-Co crowns, two parallel stainless steel (SS) archwires, and distractors.
Predistraction orthodontics
Expansion-if necessary-, leveling and aligning has to be completed before distraction. It is important to create a 2-3 mm space and root divergence between anchorage teeth and the transport teeth to allow vertical osteotomy. If lower arch needs treatment, it should also be treated before distraction stage. This is important to decide for the adequate amount of sagittal advancement. When the patient is ready for the surgery, all the bands and braces in the maxillary arch are debonded, teeth cleaned, and a thick essix plate is prepared for preserving the arch until cementation.
Appliance construction
An accurate two-step impression is taken with polyvinyl siloxane material from the debonded maxillary arch. The crowns are constructed on unprepared teeth. On the cast model, anchorage and transport units and places for tubes and the semitubes are defined and sent for wax modeling of Cr-Co crowns [Figures 1 and 2]. Usually, bilateral molar teeth are the anchorage units and they are connected with a 3-4 mm wide, 1-2 mm thick transpalatal arch to reinforce the anchorage. The orthodontist checks the wax model and makes necessary corrections before casting. Important issues at this stage are the horizontal orientation of the double-tubes and the semitubes. They all have to be positioned on the same plane for passive insertion of the archwires. Double-tubes and semitubes are the accessory units that carry and guide the customized archwires during distraction. Double-tubes are placed on the anchor unit. Semitubes are placed on the interproximal areas on the transport units. They both should have an inner diameter of 2 mm. It is also possible to cover the labial surfaces of the anterior teeth with veneer facets for a more esthetic appliance [Figure 3].
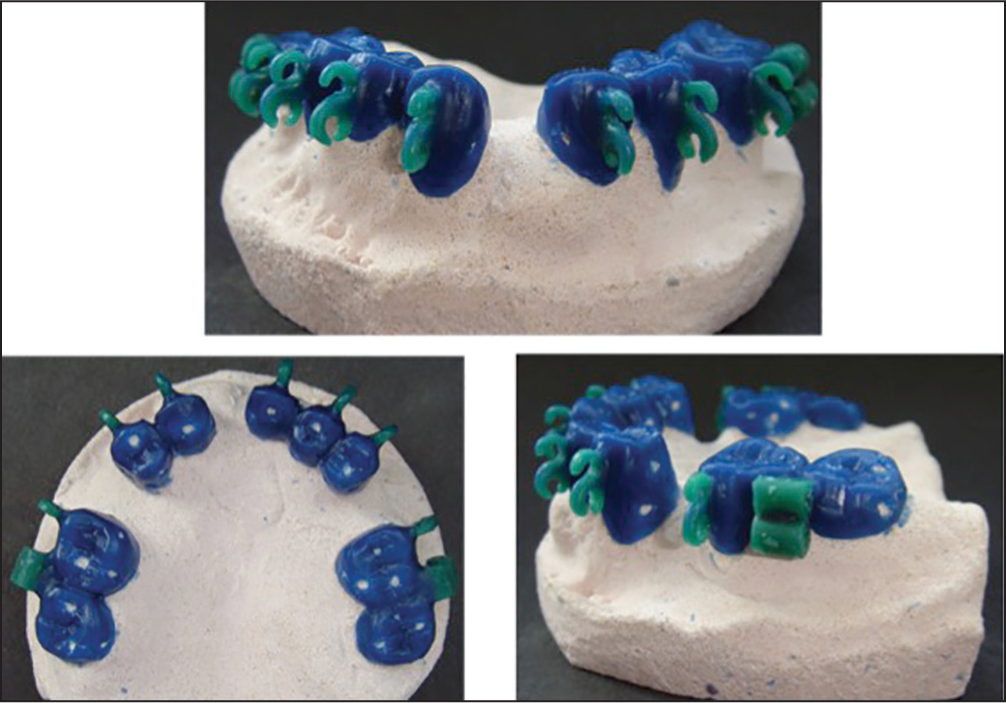
- Wax models on the model before final construction. Double-tubes and semi-tubes are seen in green wax
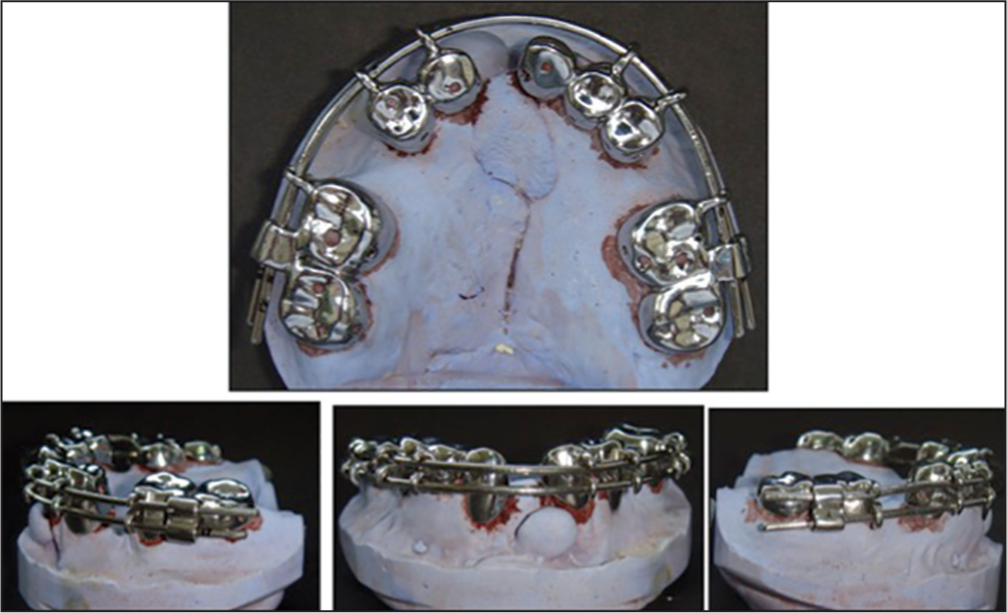
- Cr-Co crowns with the archwires placed

- Esthetic AWDA on the model, with arch-wires and distractors in place
Archwires
In AWDA, distraction progresses on two parallel archwires. When the actual crowns arrive from the laboratory, two customized archwires are bent from 1.5 mm SS wires on the model with crowns [Figure 4]. The wires must be bent according to the arch shape for passive engagement. If only transversal transport is planned in the distraction protocol, the archwires should be cinched back. If sagittal correction is a part of the distraction protocol, then some wire extension should be left distal to the double-tubes before cinching back, according to the amount of sagittal advancement. Placing the double-tubes as mesial as it is possible will help to minimize mucosal irritation due to thick archwires.

- Archwise Distraction Appliance with an expansion screw. Two archwires bent from 1.5 mm stainless steel wires
Distractor
Distractor (Tasarimmed, Istanbul, Turkey) is designed and registered by Dr. Erverdi. It has evolved a lot and reached its final small design, easily tolerated by the patient [Figures 5 and 6]. One full turn with the key creates 1 mm activation. The distractor has infinite activation ability. When the distractor reaches the maximum amount of activation, it can be closed completely and crimpable rings are crimped on the cervical archwire to accommodate the reactivation of the distractor. Before closing the distractor for reactivation, a custom made plier can be used to hold the newly formed distraction space between the teeth to prevent collapsing.

- Distractors. (a) previous design, showing activations; (b) new smaller design

- Full appliance, with activations
Cementation of the crowns
Cr-Co crowns are first checked on the teeth before final cementation. The crowns should be passive and stable on the teeth. All tubes should be on the same level. They should have small holes for the drainage of excess cement. The appliance is cemented with a dual cure glass ionomer (GIC), 1-2 days prior to the surgery.
Surgery
Surgery is performed under general anesthesia. Vertical cuts are made where the root divergence is made. Horizontal cuts are made above the apices and the segments are mobilized. Cleft area is also cleared from any irregular bony edges so that the two segments can get as close as possible. Archwires and distractors are placed during surgery after segments are mobilized. Latency period should be 5-7 days.
Distraction period
After latency, the patient begins the activation; half-turn twice a day (with 12 h interval) and the overall rate is 1 mm/day. If sagittal correction is a part of the treatment plan, it is the first objective during distraction. During activation for sagittal advancement, archwire length on the cleft area must be fixed with crimpable rings, so that, this area is preserved and segments move sagittally. When sagittal correction is achieved with 30% overcorrection; then the rings on the cleft area are removed, archwires are cinched-back to fix the arch length, and distractor is activated for lateral transport until the defect is closed with the contact of transport segment and the opposing sound alveolar bone.
Docking site surgery and consolidation
Docking site is the area where two bone segments meet. At the end of distraction, the edges of the transport bones are hypotrophic and sclerotic.[7] To close this gap and provide an intact alveolar bone bridge, docking site surgery must be performed. At the same surgery, remaining oronasal fistula can be repaired as well. It can be performed early during the consolidation period so that healing occurs simultaneously. In our procedure, consolidation period is set as minimum 6 months with AWDA. During consolidation, rigid fixation of the distracted bone is essential to prevent relapse and to allow proper calcification and solidification of the hard callus into mature bone.[4,6]
Finishing
After adequate consolidation period, the appliance is removed. The regenerated bone in the distraction site is a healthy and young bone suitable for either implant placement or orthodontic tooth mesialization. Because CLP patients usually have missing teeth due to the cleft area, implant placement, and restorations are more frequently adopted.
CASE REPORT
A 18-year-old male patient with a unilateral CLP on the left side. He had maxillary hypoplasia due to the scar tissue after labiopalatal reconstruction. After 6 months of pre-surgical orthodontic treatment, he received AWDA treatment. Distraction was planned bilaterally for the advancement of the anterior segment. Active distraction period lasted 12 days with the overcorrection. After 6 months of consolidation period, 2 implants were placed posteriorly, on the newly regenerated distraction bone. Total treatment time was 18 months. Figures 7-12 summarize the case.

- Extraoral and intraoral photos at the beginning of the treatment

- During activation of the distractors. Distraction spaces mesial to 1st molars are getting created

- (a) Initial intraoral photos; (b) during consolidation period; distraction is completed, distractors are fixed
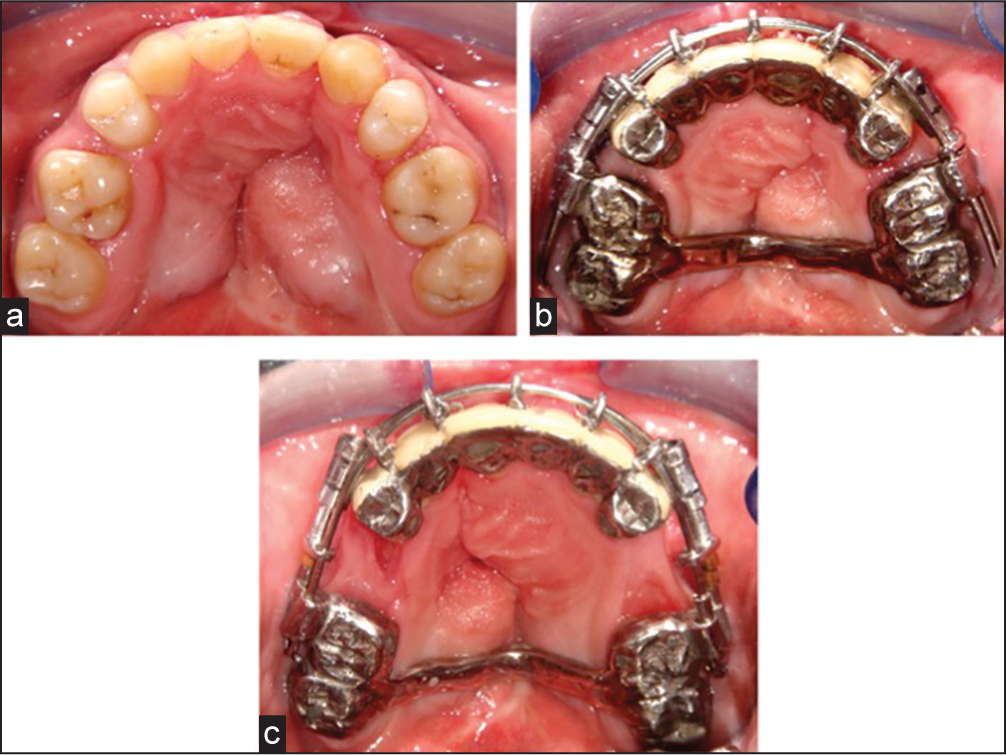
- Occlusal photos showing (a) pretreatment; (b) during distraction; (c) after distraction

- Extraoral photos before treatment, during consolidation and completion of treatment

- Panoramic radiographs and posttreatment intraoral photos (a) pretreatment, (b) during consolidation, (c) posttreatment OPTGs, (d and e) posttreatment intraoral photos
CONCLUSION
Our studies show that the AWDA is a successful appliance in cases of DO.[8,9] The only disadvantage can be the unaesthetic appearance of the appliance because of the metal casts, but veneer facets can overcome this limitation. Moreover, we clinically observed that it is well tolerated by the patients; they did not complain about esthetics during the 6-7 months’ time with the appliance.
Alveolar DO has significant advantages over conventional treatment modalities for CLP patients:
The cleft area is reduced significantly. This enables to minimize the grafting area, reduces the amount of necessary graft material, and increases the amount of bone augmentation.
Since the area is smaller, recurrent bone grafting can be eliminated. Number of surgeries is reduced.
The risk of relapse is reduced because soft tissue stresses are reduced in comparison to one-step advancement with orthognathic surgery.
More maxillary advancement is possible.
New and healthy bone is regenerated at the posterior while defect is being closed anteriorly.
Maxillary advancement can be performed in earlier ages during adolescence, and this is important to improve the facial esthetics and life quality in CLP patients in earlier stages.[7]
Velopharyngeal insufficiency problem is overcome since sagittal correction is achieved with DO of the segments mesial to molar teeth. Velopharyngeal distance is not increased at all.
Cleft lip and palate patients usually have missing teeth because of the defect area. With alveolar distraction, these missing teeth can also be restored with implants posteriorly on the newly-formed and healthy distraction bone while the cleft area is closed anteriorly.
With the rigid construction and double-arch system of AWDA, it is successful to control distraction vector for preserving the arch shape.
Distractors can be activated infinitely, and there is no need for secondary surgery to remove them.
Other than CLP, alveolar distraction with AWDA can be performed in any cases where a big alveolar defect that is not likely to be augmented with grafting exists (due to e.g., cysts, trauma, dentoalveolar retrusion, iatrogenic reasons).[10]
Acknowledgment
I thank my PhD student Dr. Yasemin Bahar Acar for her assisstance and cooperation in this paper.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- On the means of lengthening, in the lower limbs, the muscles and tissues which are shortened through deformity. J Bone Joint Surg Am. 1905;2:353-69.
- [Google Scholar]
- The tension-stress effect on the genesis and growth of tissues. Part I. The influence of stability of fixation and soft-tissue preservation. Clin Orthop Relat Res. 1989;238:249-81.
- [Google Scholar]
- The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res. 1989;239:263-85.
- [Google Scholar]
- Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res. 1990;250:8-26.
- [Google Scholar]
- Cranio-facial distraction osteogenesis: A review of the literature. Part II: Experimental studies. Int J Oral Maxillofac Surg. 2002;31:123-35.
- [Google Scholar]
- Distraction osteogenesis of the craniofacial skeleton. Plast Reconstr Surg. 2001;107:1812-27.
- [Google Scholar]
- Bone transport by distraction osteogenesis for maxillomandibular reconstruction In: Bell WH, Guerrero CA, eds. Distraction Osteogenesis of the Facial Skeleton (1st ed). Ontario: BC Decker Inc.; 2007. p. :507.
- [Google Scholar]
- A novel vector control device in horizontal bone transport. J Oral Maxillofac Surg. 2013;71:768-74.
- [Google Scholar]
- Interdental distraction osteogenesis for the management of alveolar clefts: archwise distraction. Int J Oral Maxillofac Surg. 2012;41:37-41.
- [Google Scholar]
- Special clinical conditions that AWDA can be a solution. Alveolar Distraction Osteogenesis (1st ed). New York: Springer; 2015. p. :92-8.




